|
Generalized Anxiety Disorder
"I always thought I was just
a worrier. I'd feel keyed up & unable to relax. At times it would come & go & at times it would be constant. It
could go on for days. I'd worry about what I was going to fix for a dinner party, or what would be a great present for somebody.
I just couldn't let something go.
"I'd have terrible sleeping
problems. There were times I'd wake up wired in the middle of the night. I had trouble concentrating, even reading the newspaper
or a novel. Sometimes I'd feel a little lightheaded. My heart would race or pound. And that would make me worry more. I was
always imagining things were worse than they really were: when I got a stomachache, I'd think it was an ulcer.
"When my problems were at
their worst, I'd miss work & feel just terrible about it. Then I worried that I'd lose my job. My life was miserable until
I got treatment."

Generalized anxiety disorder (GAD) is much more than the normal anxiety
people experience day to day. It's chronic & fills one's day w/ exaggerated worry & tension, even though there is little or nothing to provoke it.
Having this disorder means
always anticipating disaster, often worrying excessively about health, money, family, or work. Sometimes, though, the source of the worry is hard
to pinpoint. Simply the thought of getting thru the day provokes anxiety.
People w/GAD can't seem to shake their concerns, even though they usually realize that their anxiety is more intense
than the situation warrants.
Their worries are accompanied
by physical symptoms, especially fatigue, headaches, muscle tension, muscle aches, difficulty swallowing, trembling, twitching,
irritability, sweating & hot flashes. People w/GAD may feel lightheaded or out of breath.
They also may feel nauseated or have to go to the bathroom frequently.
Individuals w/GAD seem unable to relax & they may startle more easily than other people. They tend to have difficulty
concentrating, too. Often, they have trouble falling or staying asleep.
Unlike people w/several other
anxiety disorders, people w/GAD don't characteristically
avoid certain situations as a result of their disorder. When impairment associated w/GAD
is mild, people w/the disorder may be able to function in social settings or on the job. If severe, however, GAD can be very debilitating, making it difficult to carry out even the most ordinary daily activities.
GAD
affects about 4 million adult Americans1 & about twice as many women as men.2 The disorder comes on gradually & can begin across the life cycle, though the risk is highest between childhood
& middle age.2
It's diagnosed
when someone spends at least 6 months worrying excessively about a number of everyday problems. There's evidence that genes
play a modest role in GAD.13
GAD
is commonly treated w/medications. GAD rarely occurs alone, however; it is usually accompanied by another anxiety disorder, depression or substance abuse.2,4 These other conditions must be treated along w/GAD.

Treatment of Anxiety Disorders
Effective treatments for each
of the anxiety disorders have been developed through research.19 In general, two types of treatment are available for an anxiety disorders: medication & specific types of psychotherapy (sometimes called "talk therapy").
Both approaches can be effective
for most disorders. The choice of one or the other, or both, depends on the patient's & the doctor's preference &
also on the particular anxiety disorders.
i.e., only psychotherapy has
been found effective for specific phobias. When choosing a therapist, you should find out whether medications will be available if needed.
Before treatment can begin,
the doctor must conduct a careful diagnostic evaluation to determine whether your symptoms are due to an anxiety disorders, which anxiety disorders(s) you may have & what coexisting
conditions may be present.
Anxiety disorders aren't all
treated the same & it's important to determine the specific problem before embarking on a course of treatment. Sometimes
alcoholism or some other coexisting condition will have such an impact that it is necessary to treat it at the same time or before treating
the anxiety disorders.
If you've been treated previously
for an anxiety disorder, be prepared to tell the doctor what treatment you tried. If it
was a medication, what was the dosage, was it gradually increased & how long did you take it?
If you had psychotherapy,
what kind was it & how often did you attend sessions? It often happens that people believe they have "failed" at treatment,
or that the treatment has failed them, when in fact it was never given an adequate trial.
When you undergo treatment
for an anxiety disorder, you & your doctor or therapist will be working together as
a team. Together, you will attempt to find the approach that's best for you. If one treatment doesn't work, the odds are good
that another one will. And new treatments are continually being developed thru research. So don't give up hope.
Medications
Psychiatrists or other physicians
can prescribe medications for anxiety disorders. These doctors often work closely w/psychologists,
social workers or counselors who provide psychotherapy.
Although medications won't cure an anxiety disorder, they can keep the symptoms under control & enable you
to lead a normal, fulfilling life.
The major classes of medications used for various anxiety disorder are described below.
Antidepressants
A number of medications that
were originally approved for treatment of depression have been found to be effective for anxiety disorders. If your doctor prescribes an antidepressant,
you'll need to take it for several weeks before symptoms start to fade. So it's important not to get discouraged & stop
taking these medications before they've had a chance to work.
Some of the newest antidepressants
are called selective serotonin reuptake inhibitors, or SSRI's.
These medications act in the brain on a chemical messenger called serotonin. SSRI's tend to have fewer side effects than older antidepressants.
People do sometimes report
feeling slightly nauseated or jittery when they first start taking SSRI's, but
that usually disappears w/time. Some people also experience sexual dysfunction when taking some of these medications. An adjustment
in dosage or a switch to another SSRI will usually correct bothersome problems.
It's important to discuss
side effects w/your doctor so that he or she will know when there is a need for a change in medication.
Fluoxetine,
sertraline, fluvoxamine, paroxetine
& citalopram are among the SSRI's commonly
prescribed for panic disorder, OCD, PTSD & social phobia. SSRI's are often used
to treat people who have panic disorder in combination w/OCD, social phobia, or depression. Venlafaxine, a drug closely related to the SSRI's,
is useful for treating GAD.
Other newer antidepressants
are under study in anxiety disorders, although one, bupropion,
doesn't appear effective for these conditions. These medications are started at a low dose & gradually increased until
they reach a therapeutic level.
Similarly, antidepressant medications called tricyclics are started at low doses & gradually increased. Tricyclics have been
around longer than SSRI's & have been more widely studied for treating anxiety disorders.
For anxiety
disorders other than OCD, they're as effective as the SSRI's, but many physicians & patients prefer the newer
drugs because the tricyclics sometimes cause dizziness, drowsiness, dry mouth & weight
gain.
When these problems persist
or are bothersome, a change in dosage or a switch in medications may be needed.
Tricyclics
are useful in treating people w/co-occurring anxiety disorders & depression. Clomipramine, the only antidepressant in its class prescribed for OCD & imipramine, prescribed for panic disorder & GAD, are examples of tricyclics.
Monoamine
oxidase inhibitors, or MAOIs, are the oldest class of antidepressant medications. The most commonly prescribed MAOI is phenelzine, which is helpful for people w/panic disorder & social phobia. Tranylcypromine & isoprocarboxazid are also used to treat anxiety disorders.
People who take
MAOI's are put on a restrictive diet because these medications can interact w/some foods
& beverages, including cheese & red wine, which contain a chemical called tyramine.
MAOI's
also interact w/some other medications, including SSRI's. Interactions between MAOI's & other substances can cause dangerous elevations in blood pressure or other potentially life-threatening
reactions.
Anti-Anxiety Medications
High-potency
benzodiazepines relieve symptoms quickly & have few side effects, although drowsiness can be a problem.
Because people can develop a tolerance to them & would have to continue increasing the dosage to get the same effect,
benzodiazepines are generally prescribed for short periods of time.
One exception is panic disorder, for which they may be used for 6 months to a year. People who have had problems w/drug or alcohol abuse aren't usually good candidates for these medications because they may become dependent
on them.
Some people experience withdrawal
symptoms when they stop taking benzodiazepines, although reducing the dosage gradually can
diminish those symptoms. In certain instances, the symptoms of anxiety can rebound after these medications are stopped. Potential
problems w/benzodiazepines have led some physicians to shy away from using them, or to use them in inadequate doses, even
when they're of potential benefit to the patient.
Benzodiazepines include clonazepam, which is used for social phobia & GAD; alprazolam, which is helpful for panic disorder & GAD; & lorazepam, which is also useful for
panic disorder.
Buspirone,
a member of a class of drugs called azipirones, is a newer anti-anxiety medication that
is used to treat GAD . Possible side effects include dizziness, headaches & nausea.
Unlike the benzodiazepines, buspirone must be taken consistently for at least two weeks
to achieve an anti-anxiety effect.
Other Medications
Beta-blockers,
such as propanolol, are often used to treat heart conditions but have also been found to
be helpful in certain anxiety disorders, particularly in social
phobia. When a feared situation, such as giving an oral presentation, can be predicted in advance, your doctor may
prescribe a beta-blocker that can be taken to keep your heart from pounding, your hands
from shaking & other physical symptoms from developing.
Taking Medications
Before taking medication
for an anxiety disorder:
- Ask your doctor to tell you about the effects & side effects
of the drug he or she is prescribing.
- Tell your doctor about any alternative therapies or over-the-counter
medications you're using.
- Ask your doctor when & how the medication will be stopped.
Some drugs can't safely be stopped abruptly; they have to be tapered slowly under a physician's supervision.
- Be aware that some medications are effective in anxiety disorders
only as long as they are taken regularly & symptoms may occur again when the medications are discontinued.
- Work together w/your doctor to determine the right dosage of
the right medication to treat your anxiety disorder.
Psychotherapy
Psychotherapy involves talking w/a trained mental health professional, such as a psychiatrist, psychologist, social worker, or counselor
to learn how to deal w/problems like anxiety disorders.
Cognitive-Behavioral & Behavioral Therapy
Research has shown that a
form of psychotherapy that's effective for several anxiety disorders, particularly panic disorder & social phobia, is cognitive-behavioral therapy (CBT). It has two components.
The cognitive component helps people change thinking patterns that keep
them from overcoming their fears.
i.e., a person w/panic disorder might be helped to see that his or her panic attacks aren't really heart attacks as previously
feared; the tendency to put the worst possible interpretation on physical symptoms can be overcome.
Similarly, a person w/social phobia might be helped to overcome the belief that others are continually watching &
harshly judging him or her.
The behavioral
component of CBT seeks to change people's reactions to anxiety-provoking situations. A key element of this component is exposure,
in which people confront the things they fear.
i.e., a treatment approach
called exposure & response prevention for people w/OCD. If the person has a fear of dirt & germs, the therapist may encourage them to dirty their hands, then go a certain period
of time without washing.
The therapist helps the patient
to cope w/the resultant anxiety. Eventually, after this exercise has been repeated a number of times, anxiety will diminish.
In another sort of exposure
exercise, a person w/social phobia may be encouraged to spend time in feared social situations w/out giving in to the temptation to flee.
In some cases the individual
w/social phobia will be asked to deliberately make what appear to be slight social blunders & observe other people's reactions; if they're
not as harsh as expected, the person's social anxiety may begin to fade.
For a person w/PTSD, exposure might consist of recalling the traumatic event in detail, as if in slow motion & in effect re-experiencing
it in a safe situation. If this is done carefully, w/support from the therapist, it may be possible to defuse the anxiety
associated w/the memories.
Another behavioral technique
is to teach the patient deep breathing as an aid to relaxation & anxiety management.
Behavioral therapy alone,
w/out a strong cognitive component, has long been used effectively to treat specific phobias. Here also, therapy involves exposure. The person is gradually exposed to the object or situation that is feared.
At first, the exposure may
be only thru pictures or audiotapes. Later, if possible, the person actually confronts the feared object or situation. Often
the therapist will accompany him or her to provide support & guidance.
If you undergo CBT or behavioral
therapy, exposure will be carried out only when you are ready; it'll be done gradually & only w/your permission. You'll
work w/the therapist to determine how much you can handle & at what pace you can proceed.
A major aim of CBT & behavioral
therapy is to reduce anxiety by eliminating beliefs or behaviors that help to maintain the anxiety
disorder.
i.e., avoidance of a feared
object or situation prevents a person from learning that it is harmless. Similarly, performance of compulsive rituals in OCD gives some relief from anxiety & prevents the person from testing rational thoughts about danger, contamination, etc.
To be effective, CBT or behavioral
therapy must be directed at the person's specific anxieties. An approach that is effective for a person w/a specific phobia about dogs isn't going to help a person w/OCD who has intrusive thoughts of harming loved ones.
Even for a single disorder,
such as OCD it's necessary to tailor the therapy to the person's particular concerns. CBT & behavioral therapy have no adverse side
effects other than the temporary discomfort of increased anxiety, but the therapist must be well trained in the techniques
of the treatment in order for it to work as desired.
During treatment, the therapist
probably will assign "homework"—specific problems that the patient will need to work on between sessions.
CBT or behavioral therapy
generally lasts about 12 weeks. It may be conducted in a group, provided the people in the group have sufficiently similar
problems.
Group therapy is particularly
effective for people w/social phobia. There's some evidence that, after treatment is terminated,
the beneficial effects of CBT last longer than those of medications for people w/panic disorder; the same may be true for OCD, PTSD & social phobia.
Medication may be combined w/psychotherapy & for many people this is the best approach to treatment. As stated earlier, it's important
to give any treatment a fair trial. And if one approach doesn't work, the odds are that another one will, so don't give up.
If you've recovered from an
anxiety disorder & at a later date it recurs, don't consider yourself a "treatment failure."
Recurrences can be treated effectively, just like an initial episode.
In fact, the skills you learned
in dealing w/the initial episode can be helpful in coping w/a setback.
Beyond shyness: Overcoming the fear of social situations By Mayo Clinic staff
Everyone feels nervous from time to time. Going on a first date or giving a speech often causes that butterflies-in-your-stomach feeling. Or you may initially feel shy at a party
among a group of strangers, but then warm up to them.
For some people, though, this
sort of normal nervousness is magnified into extreme fear &
anxiety. They avoid dating, giving speeches or attending parties altogether. They fear being watched or humiliated
while doing something in front of others.
Everyday social activities,
even the most mundane, may become virtually impossible. You may not even be able to eat w/others or sign a personal check
in public.
When social
anxieties become this extreme & disrupt your life, interfere w/education or work & lead you to avoid certain
situations, they may have crossed the line into a condition known as social phobia. (also called
social anxiety disorder)
"Social phobia can severely limit dating, academic achievement & career choice," notes Lois Krahn,
M.D., a psychiatrist at Mayo Clinic in Scottsdale, Ariz. "It can disrupt much of life's activity."
But the right treatment —
counseling, behavioral techniques & medication — can improve the quality of life & open up opportunities that the fear & anxiety had shut out.
Social
phobia, sometimes called social anxiety disorder, isn't the same as shyness or so-called
stage fright. In fact, sometimes it's perfectly reasonable to have some fear in certain social situations.
If you're afraid of being called on in class or at a meeting because you haven't prepared, that's appropriate apprehension or even fear, not social phobia. On the other hand, turning down a job that requires public speaking
could be an indication of social phobia.
Similarly, getting the jitters
opening night in your first community theater production is normal fear. Avoiding the theater altogether, even if you love it, because you believe others may be critical, could be social phobia.
Sometimes, you may be able
to force yourself to endure such events, but only after dreading them for weeks beforehand. During the event, or even for
days leading up to it, you may have intense anxiety & a variety of physical reactions,
such as:
- sweating
- blushing
- tremors
- diarrhea
- stomach upset
Even the worry about having
these signs & symptoms in public can heighten your anxiety and fear, which, in turn, worsens them — a vicious cycle.
Common, everyday experiences
can be a source of social phobia:
- Using a public restroom or telephone
- Returning items to a store
- Interacting w/strangers or w/people of the opposite sex
- Writing in front of others
- Making eye contact
- Entering a room in which people are already seated
- Ordering food in a restaurant
- Being introduced to strangers
"These situations are extremely challenging for people w/social phobia because they
feel painfully self-conscious," Dr. Krahn explains.
"They believe that others
are watching them & expect them to harbor critical thoughts about them. They may feel that onlookers are critical of what
they're doing, how they're doing it, what they're wearing & what they're saying to the point that they can't engage in
a fairly simple activities:
i.e., talking to a clerk when
people are lined up nearby waiting."
Some of the features that
suggest true social phobia rather than normal shyness or reserve:
- An intense & persistent fear of social or performance situations
in which you may not know people or may be judged
- Avoiding the social situations you fear
- Fear of being embarrassed or humiliated
- Fear that others will notice you blushing, sweating, trembling
or showing other signs of anxiety
- The avoidance or distress interferes w/your life
- Recognizing that your fear is excessive or unreasonable for
the situation
There
are two types of social phobia. In global social phobia, you have trouble w/virtually
all social situations.
In specific
social phobia, you have trouble only w/a few situations. Together, both types affect about 4% of U.S. adults, or slightly
more than 5 million people.
In either case, social phobia can be debilitating. It can prevent you from making friends and limit your career or educational
opportunities. It can be a risk factor for other health problems, such as substance abuse or excessive drinking in an attempt to cope. And it can also lead to depression or suicide.
Social
phobia tends to begin in childhood or early adolescence.
Although it typically persists for life, often waxing & waning, treatment can help you control it.
The two most effective types
of treatment are psychotherapy & medications, often in combination.
Therapy is often a form called
cognitive behavioral therapy. It's based on the premise that your own thoughts — not other people or situations — determine how you behave
or react. Even if an unwanted situation hasn't changed — you still have to give that presentation to management, for
instance — you can change the way you think & behave in a positive way.
Therapy may also include exposure therapy, in which you face the situations you fear most & gradually become better skilled in coping w/them. And you may also
participate in skills training or role playing to practice your social skills & gain comfort relating to others.
Numerous types of medications may help social phobia, since the condition may be associated
w/a chemical imbalance in the brain. The Food & Drug Administration, however, has specifically approved only three
medications to treat social phobia:
-
Paroxetine. Paroxetine (Paxil,
Paxil CR) is a type of antidepressant called a selective serotonin reuptake inhibitor (SSRI).
SSRI's help balance out a brain chemical called serotonin, which can help relieve symptoms
of social phobia. Side effects may include nausea, diarrhea, decreased appetite, sweating, abnormal vision & sexual problems.
- Sertraline.
Sertraline (Zoloft) is also an SSRI. Its most common side effects include upset stomach,
sleeping difficulties, diarrhea, dry mouth, sexual problems, feeling sleepy or tired, tremor, sweating, agitation & decreased
appetite.
- Venlafaxine.
Venlafaxine (Effexor) is a type of antidepressant called a serotonin & norepinephrine reuptake inhibitor (SNRI). It helps to balance out both serotonin
& another brain chemical, norepinephrine. Common side effects include nausea, dizziness, sleepiness, delayed ejaculation,
sweating, dry mouth, insomnia, anorexia & constipation.
For some people, the symptoms
of social phobia may fade over time & medication can be discontinued. Others may have
to take medication for years to prevent a relapse.
Which medication, if any,
is best for you depends on your situation. Talk to your doctor about whether medications are right for you.
|
 |
|
Coexisting Conditions
It's common for an anxiety disorder to be accompanied by another anxiety disorder or another
illness.4,5,6 Often people who have panic disorder or social phobia, i.e., also experience the intense sadness & hopelessness associated w/depression. Other conditions that a person can have along w/an anxiety disorder include an eating disorder or alcohol or drug abuse. Any of these problems will need to be treated as well, ideally at the same time as the anxiety
disorder.
How to Get Help for Anxiety Disorders
If you, or someone you know,
has symptoms of anxiety, a visit to the family physician is usually the best place to start.
A physician can help determine whether the symptoms are due to an anxiety disorder, some other medical condition, or both. Frequently,
the next step in getting treatment for an anxiety disorder is referral to a mental health
professional.
Among the professionals who
can help are psychiatrists, psychologists, social workers & counselors. However, it's best to look for a professional
who has specialized training in cognitive-behavioral therapy &/or behavioral therapy, as appropriate & who is open to the use of medications, should they be needed.
As stated earlier, psychologists,
social workers & counselors sometimes work closely w/a psychiatrist or other physician, who'll prescribe medications when
they're required. For some people, group therapy is a helpful part of treatment.
It's important that you feel
comfortable w/the therapy that the mental health professional suggests. If this isn't the case, seek help elsewhere. However,
if you've been taking medication, it's important not to discontinue it abruptly, as stated before. Certain drugs have to be
tapered off under the supervision of your physician.
Remember, though, that when
you find a health care professional that you're satisfied with, the 2 of you are working together as a team. Together you'll
be able to develop a plan to treat your anxiety disorder that may involve medications, cognitive-behavioral or other talk
therapy, or both, as appropriate.
You may be concerned about
paying for treatment for an anxiety disorder. If you belong to a Health Maintenance Organization (HMO) or have some other
kind of health insurance, the costs of your treatment may be fully or partially covered. There are also public mental health
centers that charge people according to how much they're able to pay. If you're on public assistance, you may be able to get
care thru your state Medicaid plan.
Strategies To Make
Treatment More Effective
Many people w/anxiety disorders benefit from joining a self-help group & sharing their problems & achievements w/others.
Talking w/trusted friends or a trusted member of the clergy can also be very helpful, although not a substitute for mental
health care.
Participating in an Internet
chat room may also be of value in sharing concerns &decreasing a sense of isolation, but any advice received should be
viewed w/caution.
The family is of great importance
in the recovery of a person w/an anxiety disorder. Ideally, the family should be supportive
w/out helping to perpetuate the person's symptoms. If the family tends to trivialize the disorder or demand improvement without
treatment, the affected person will suffer.
You may wish to show this informationa to your family &
enlist their help as educated allies in your fight against your anxiety disorder.
Stress management techniques & meditation may help you to calm yourself & enhance the effects of therapy, although there is
as yet no scientific evidence to support the value of these "wellness" approaches to recovery from anxiety disorders.
There is preliminary evidence
that aerobic exercise may be of value & it's known that caffeine, illicit drugs & even some over-the-counter cold
medications can aggravate the symptoms of an anxiety disorder. Check w/your physician or
pharmacist before taking any additional medicines.
|
|
|
|
|
Role of Research in
Improving the Understanding & Treatment of Anxiety Disorders
NIMH supports research into
the causes, diagnosis, prevention & treatment of anxiety disorders & other mental illnesses. Studies examine the genetic & environmental risks for major anxiety disorders,
their course, both alone & when they occur along w/other diseases such as depression & their treatment.
The ultimate goal is to be
able to cure & perhaps even to prevent, anxiety disorders.
NIMH is harnessing the most sophisticated
scientific tools available to determine the causes of anxiety disorders. Like heart disease
& diabetes, these brain disorders are complex & probably result from a combination of genetic, behavioral, developmental
& other factors.
Several parts of the brain
are key actors in a highly dynamic interplay that gives rise to fear & anxiety.14 Using brain imaging technologies & neurochemical techniques, scientists are finding that a network of interacting
structures is responsible for these emotions.
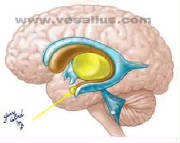
Much research centers on the
amygdala, an almond-shaped structure deep within the brain. The
amygdala is believed to serve as a communications hub between the parts of the brain that process incoming sensory signals
& the parts that interpret them.
It can signal that a threat
is present & trigger a fear response or anxiety. It appears that emotional memories stored in the central part of the amygdala
may play a role in disorders involving very distinct fears, like phobias, while different parts may be involved in other forms of anxiety.
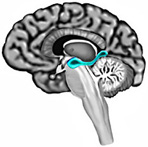
Other research focuses on
the hippocampus, another brain structure that is responsible for
processing threatening or traumatic stimuli. The hippocampus plays a key role in the brain by helping to encode information
into memories.
Studies have shown that the
hippocampus appears to be smaller in people who have undergone
severe stress because of child abuse or military combat.15,16 This reduced size could help explain why individuals w/PTSD have flashbacks, deficits in explicit memory & fragmented memory for details of the traumatic event.
Also, research
indicates that other brain parts called the basal ganglia & striatum
are involved in obsessive-compulsive disorder.17
By learning more about brain
circuitry involved in fear & anxiety, scientists may be able to devise new & more specific treatments for anxiety
disorders.
For example, it someday may
be possible to increase the influence of the thinking parts of the brain on the amygdala, thus placing the fear & anxiety
response under conscious control. In addition, w/new findings about neurogenesis (birth of new
brain cells) throughout life,18 perhaps a method will be found to stimulate growth of new neurons in the hippocampus
in people w/PTSD.
NIMH-supported studies of
twins & families suggest that genes play a role in the origin of anxiety disorders.
But heredity alone can't explain what goes awry. Experience also plays a part. In PTSD, for example, trauma triggers the anxiety disorder; but genetic factors may explain why only certain individuals
exposed to similar traumatic events develop full-blown PTSD.
Researchers are attempting
to learn how genetics & experience interact in each of the anxiety disorders—information
they hope will yield clues to prevention & treatment.
Scientists supported by NIMH
are also conducting clinical trials to find the most effective ways of treating anxiety disorders.
For example, one trial is examining how well medication & behavioral therapies work together & separately in the treatment
of OCD.
Another trial is assessing
the safety & efficacy of medication treatments for anxiety disorders in children & adolescents with co-occurring attention deficit hyperactivity disorder (ADHD). For more information about these & other clinical trials, visit the NIMH clinical trials web page, click here or the National Library of Medicine's clinical trials database,
www.clinicaltrials.gov.
Childhood Anxiety Often
Precedes Eating Disorders
Reuters Health / By Amy Norton / Thursday, December 9, 2004
NEW YORK (Reuters Health)
- Many women w/eating disorders may have a history of childhood anxiety
disorders, particularly social phobia & obsessive-compulsive disorder, according to a new study.
The findings, say researchers,
suggest that childhood anxiety may signal a vulnerability to the development of anorexia or bulimia.
It has long been noted that
eating disorders often co-exist w/other psychological problems, including anxiety & depression. Some small studies have also suggested that when anxiety disorders arise, they typically precede
the onset of anorexia or bulimia.
This latest study is by far
the largest to look at the issue, lead author Dr. Walter H. Kaye told Reuters Health, and the findings confirm & extend
those from previous research.
Better understanding of the
role of anxiety could improve the treatment of eating disorders,
according to Kaye, a psychiatrist at the University of Pittsburgh Medical Center. It could also aid in getting at the biological
roots of eating disorders, as the conditions may share some of their genetic underpinnings
w/anxiety disorders.
"We're ultimately looking
for genes," Kaye said, noting that he & his colleagues are recruiting people for an international study aimed at uncovering
the genes that contribute to anorexia. The researchers need to find families in which at
least two members have had anorexia.
The current study, published
in the December issue of the American Journal of Psychiatry, included 672 individuals, nearly all women, who currently or
in the past had anorexia, bulimia or both. A group of
healthy women the same age was included for comparison. All of the study participants completed standard questionnaires used
to gauge their lifetime incidence of various anxiety disorders.
Kaye & his colleagues
found that nearly 2/3 of the eating disorder patients had ever had an anxiety disorder, occurring in the majority of cases before the onset of the eating disorder.
Of the entire group, 23% were
diagnosed as having had obsessive-compulsive disorder (OCD) during childhood, before the onset of anorexia or bulimia.
Similarly, social phobia arose early on for 13%.
OCD is characterized by recurrent, intrusive thoughts & a compulsion to perform certain rituals, such as constant
hand washing or repeatedly checking that doors are locked. Social phobi is marked by an intense fear of being embarrassed or judged by others in social situations; children w/the disorder may be excessively shy & want to avoid school & activities.
According to Kaye &
his colleagues, the high rate of childhood OCD -- seen in nearly 1/4 of the eating disorder patients, compared w/the typical population
rate of 2 to 3% -- was "most striking."
It's possible, Kaye said,
that the findings could eventually help in identifying children at particular risk of developing
anorexia or bulimia.
SOURCE: American Journal of Psychiatry, December 2004.
Anxiety Disorders In Children: Parent Training Could Help
Special skills workshops for parents of anxious young children
could offer a breakthrough in addressing this difficult problem, according to psychologists at The University of Manchester.
Providing psychological treatments for children under ten with anxiety disorders is problematic for health professionals,
as the approaches that are most successful with teenagers and adults are difficult to apply to the very young.
According
to researcher Dr Samantha Cartwright-Hatton: "A treatment like cognitive behaviour therapy (CBT) relies on the patient having
highly-developed verbal skills, and needs them to understand and reflect on the causes of their symptoms. This is very difficult
for younger children, and there is not much evidence that it works with them."
The team is therefore investigating
a new approach, which allows parents to be much more involved. "Parents raising an anxious child need a very special set of
skills which nobody ever teaches you," Dr Cartwright-Hatton explains, "so we're trying out a course which helps them develop
the skills to give their child the best chance of becoming a confident, mature adult."
The team is eager to hear from
parents of children under ten who display symptoms of anxiety, such as extreme fears, phobias, frequent worry or distress
at separating from their parents. If they participate in the study they will either undertake a weekly two-hour session for
ten weeks (starting September) at the Wellcome Trust Clinical Research Facility on Grafton Street in Manchester, or receive
a thorough assessment and detailed advice on how to get the right help for their child.
Helping parents develop strategies
to both manage their children's problems and help them overcome them has already proved very successful with behavioural problems,
with even TV "infotainment" programmes being shown to be a valuable aid. In adapting the approach for anxiety disorders, Dr
Cartwright-Hatton hopes that similar benefits will result for the children suffering from them.
"Parents who have
already completed the course say they have found it enjoyable and useful, and would recommend it to others," she says. "The
therapists are very easy to talk to and the course is designed to be fun - there's no point in being all 'doom and gloom'
about these things as people learn new skills best when they are relaxed. So we make sure that we have plenty of laughs along
the way."
The course covers techniques for raising children's self-esteem and dealing with fears and worries, as well
as offering strategies for managing difficult behaviours like tantrums calmly.
"Child anxiety can carry on into adulthood
and stay with people throughout their lives, so we are starting to realise how important it is to sort it out early," Dr Cartwright-Hatton
concludes. "Successful treatment could significantly reduce adult anxiety and depression and the behaviours associated with
them, which would bring huge benefits for the health and happiness of the population as a whole, as well as for the workforce
and economy."
----------------------------
Article adapted by Medical News Today from original press
release.
----------------------------
Three Effective Treatments For Childhood Anxiety Disorders Identified By Study
Treatment that combines a certain type of psychotherapy with
an antidepressant medication is most likely to help children with anxiety disorders, but each of the treatments alone is also
effective, according to a new study funded by the National Institutes of Health's National Institute of Mental Health (NIMH).
The study was published online Oct. 30, in the New England Journal of Medicine.
"Anxiety disorders are among
the most common mental disorders affecting children and adolescents. Untreated anxiety can undermine a child's success in
school, jeopardize his or her relationships with family, and inhibit social functioning," said NIMH Director Thomas R. Insel,
M.D. "This study provides strong evidence and reassurance to parents that a well-designed, two-pronged treatment approach
is the gold standard, while a single line of treatment is still effective."
The Child/Adolescent Anxiety Multimodal
Study (CAMS) randomly assigned 488 children ages 7 years to 17 years to one of four treatment options for a 12-week period:
- Cognitive behavioral therapy (CBT), a specific type of therapy
that, for this study, taught children about anxiety and helped them face and master their fears by guiding them through structured
tasks;
- The antidepressant sertraline (Zoloft), a selective serotonin
reuptake inhibitor (SSRI);
- CBT combined with sertraline;
- pill placebo (sugar pill).
The children, recruited from six regionally dispersed sites
throughout the United States, all had moderate to severe separation anxiety disorder, generalized anxiety disorder or social
phobia. Many also had coexisting disorders, including other anxiety disorders, attention deficit hyperactivity disorder, and
behavior problems.
John Walkup, M.D., of Johns Hopkins Medical Institutions, and colleagues found that among those
in combination treatment, 81 percent improved. Sixty percent in the CBT-only group improved, and 55 percent in the sertraline-only
group improved. Among those on placebo, 24 percent improved. A second phase of the study will monitor the children for an
additional six months.
"CAMS clearly showed that combination treatment is the most effective for these children. But
sertraline alone or CBT alone showed a good response rate as well. This suggests that clinicians and families have three good
options to consider for young people with anxiety disorders, depending on treatment availability and costs," said Walkup.
Results also showed that the treatments were safe. Children taking sertraline alone showed no more side effects than
the children taking the placebo and few children discontinued the trial due to side effects. In addition, no child attempted
suicide, a rare side effect sometimes associated with antidepressant medications in children.
CAMS findings echo previous
studies in which sertraline and other SSRIs were found to be effective in treating childhood anxiety disorder. The study's
results also add more evidence that high-quality CBT, with or without medication, can effectively treat anxiety disorders
in children, according to the researchers.
"Further analyses of the CAMS data may help us predict who is most likely
to respond to which treatment, and develop more personalized treatment approaches for children with anxiety disorders," concluded
Philip C. Kendall, Ph.D., of Temple University, a senior investigator of the study. "But in the meantime, we can be assured
that we already have good treatments at our disposal."
----------------------------
Article adapted by Medical
News Today from original press release.
----------------------------
The six CAMS sites were Duke University;
New York State Psychiatric Institute/Columbia University Medical Center; Johns Hopkins University; Temple University/University
of Pennsylvania; University of California, Los Angeles; and the Western Psychiatric Institute and Clinic/University of Pittsburgh
Medical Center.
The National Institute of Mental Health (NIMH) mission is to reduce the burden of mental and behavioral
disorders through research on mind, brain, and behavior. More information is available at the NIMH website, http://www.nimh.nih.gov/.
The National Institutes of Health (NIH) - The Nation's
Medical Research Agency - includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human
Services. It is the primary federal agency for conducting and supporting basic, clinical and translational medical research,
and it investigates the causes, treatments, and cures for both common and rare diseases. For more information about NIH and
its programs, visit http://www.nih.gov/.
Reference: Walkup JT, Albano AM, Piacentini J, Birmaher
B, Compton SN, Sherrill J, Ginsburg GS, Rynn MA, McCracken J, Waslick B, Iyengar S, March JS, Kendall PC. Cognitive-behavioral
therapy, sertraline and their combination for children and adolescents with anxiety disorders: acute phase efficacy and safety.
New England Journal of Medicine. Online ahead of print 30 Oct 2008: 359(17).
Source: Colleen Labbe
NIH/National Institute of Mental Health
source site: click here
|
|
|
|
|
|
|
|




